Ebola – Fordham Now
https://now.fordham.edu
The official news site for Fordham University.Fri, 11 Dec 2015 23:42:16 +0000en-US
hourly
1 https://now.fordham.edu/wp-content/uploads/2015/01/favicon.pngEbola – Fordham Now
https://now.fordham.edu
3232232360065Healing Ebola
https://now.fordham.edu/fordham-magazine/healing-ebola/
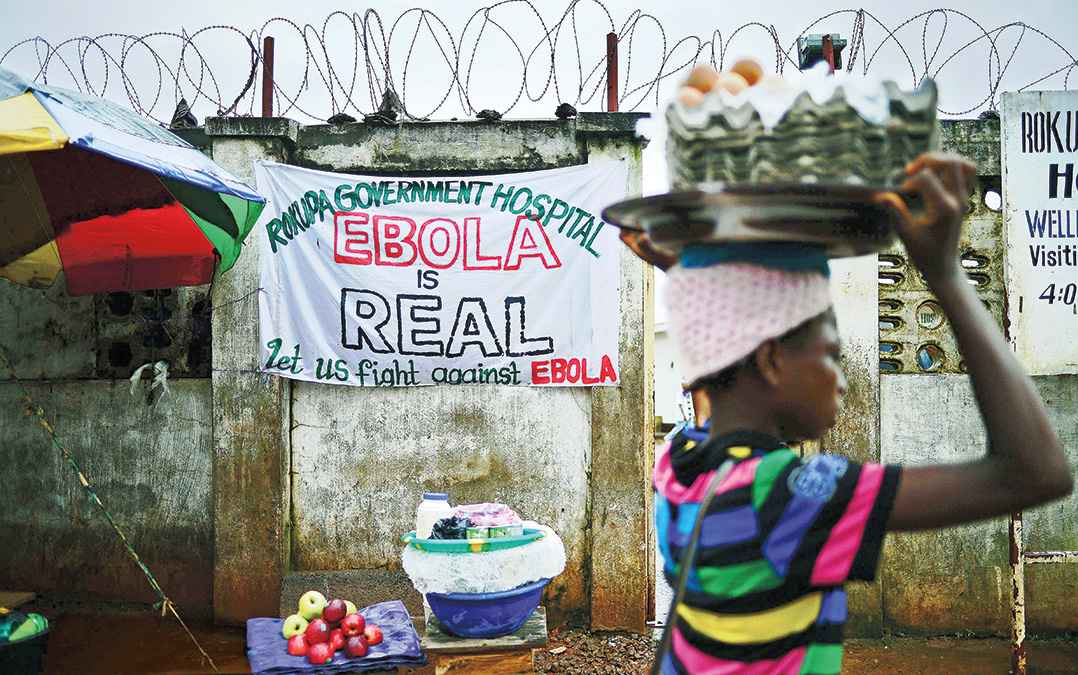
Fri, 11 Dec 2015 23:42:16 +0000http://news.fordham.sitecare.pro/?p=34296A woman walks past an Ebola warning sign outside a government hospital in Freetown, Sierra Leone, in August 2014. Carl De Souza/AFP/Getty Images
What happens when a global health crisis leaves the Western media spotlight?
The Ebola virus, as seen under a microscope
As he watched a patient he’d grown close to die at one of Mother Teresa’s homes for the terminally ill in Kolkata, Joseph Woodring, DO, FCRH ’98, felt overwhelmed by his inability to help the man—and he had an epiphany. “I’d been holding his hand, watching his chest rise and fall,” said Woodring, who first visited India in 1995 as an undergraduate in Fordham’s Global Outreach program. On that trip, he learned to connect with suffering and honor the human dignity of sick and impoverished people. But now, a few years out of college, he wanted to examine the bigger picture. “If I don’t get upstream and learn what these guys have,” he thought, “I’m not fixing anything. I want to be able to actually treat people.”
Last year, during the Ebola outbreak in West Africa, Woodring deployed to Liberia as an epidemiologist for the Centers for Disease Control and Prevention. His job was to trace the spread of the virus and work with local people to arrest the contagion. By showing respect for the dignity and self-determination of people in the villages, he said, he was able to convince communities to adopt practices that stopped the spread of Ebola.
Now back in New York, Frazier, an adjunct instructor at Fordham’s Institute of International Humanitarian Affairs, stresses that recovering from the outbreak will require sustained international attention and sincere collaboration with affected communities. Emergency Ebola treatment centers are being turned into permanent clinics. That’s good, Frazier said, but villages will also have to reintegrate stigmatized Ebola survivors, negotiate what to do with the land of families wiped out by Ebola, find a way to care for and pay school fees for orphaned children, and address other consequences not yet identified.
“The immediate emergency seems to have subsided, but now what? The tendency with media and some humanitarians is OK, done. But for there to be full-on economic recovery, it is going to take a lot of time,” she said, and “it needs to be bottom up.”
The first case of the most recent Ebola outbreak was reported in March 2014 in Guinea. By August, the United Nations Health Agency had labeled the outbreak an international public health emergency, as the disease galloped across Liberia, Sierra Leone, and Guinea, swallowing thousands of victims and decimating those nations’ small and dedicated cadre of medical professionals.
More than 11,000 people died. For eight months, the response was left to just two international charities: Doctors Without Borders and Samaritan’s Purse. While they did heroic frontline medical work, they and later arrivals were ill-equipped to halt the spread of the disease. They had a hard time convincing people to stop kissing or shaking hands, and to suspend traditional burial practices that involve washing and caressing the body—expressions of deeply held spiritual beliefs but also certain methods for communicating the disease.
Medical response teams full of foreigners wrapped in bright yellow plastic suits with shields over their faces arrived on trucks in remote villages to remove the bodies of the dead. They were met with resistance and fear. People hid their sick relatives and buried the dead secretly, allowing the disease to blossom.
Epidemiologist Joseph Woodring, DO, FCRH ’98 (left), in Liberia last year.
When he arrived in Liberia in October, Woodring realized a different approach would be necessary. He focused on communicating with people who could effect change. “It’s the village elders that made the impact,” he said, by enforcing quarantines and maintaining the 21-day observation of anyone directly exposed to the disease. “The village elders were at the apex of those societies, and [people]were roaring in and stripping them of their traditional role. We had to go to the elders and work with them. You’d inform traditional healers and give them due deference and tell them, look, this practice is very dangerous.”
Collaborating with local social systems is key, experts say, both for effective containment of diseases and to lay the groundwork for recovery. Thousands of foreign nurses, doctors, and aid workers, among them several Fordham alumni and staff, aided their West African counterparts during the Ebola outbreak. A year later, the disease is nearly abated, and Western media, which fueled hysteria and panic in the United States during the outbreak, has shifted to other crises. But the affected countries are still struggling to recover, and humanitarian experts are studying the Ebola outbreak to learn how the world can respond sooner and better—and even prevent the next disaster.
The solutions are straightforward but terribly difficult to achieve, according to Alexander van Tulleken, MD, senior fellow at Fordham’s Institute of International Humanitarian Affairs. “The next pandemic is prevented by building a world where people are given the opportunity to get educated and thrive,” he said. It might sound trite, but he’s serious. A strong healthcare system, access to education, and a stable civil society are what ultimately protect against disease.
The reason Ebola was so deadly and persistent in Liberia, Sierra Leone, and Guinea, while cases elsewhere were more quickly contained, has everything to do with the destabilizing effects of war and extreme poverty. “Diseases are opportunists,” Van Tulleken said. “They only thrive in certain climates. Like criminals and terrorists, they look for places where rule of law is broken down.”
With national infrastructure—not just roads but electrical systems, healthcare, communication, and trust in government—broken apart by years of armed conflict and underinvestment, fighting Ebola was especially difficult, said Melissa Labonte, PhD, an associate professor of political science at Fordham, who has studied the region extensively. She said doctors focused on a medical and technical response, but social wounds allowed Ebola to fester, so a social response was also needed to beat it back.
“You can’t go in and just do things. The imperative is to respond, I know, but you have to know what you are doing before you start acting,” Labonte said. “Local knowledge matters. It was undervalued. Once we started to listen to it and value it, things changed for the better.”
Health and humanitarian experts say collaborating with local social systems is key to halting the spread of the Ebola virus.
Because the virus is strongest at and even after death, people who care for the sick and prepare the deceased for burial are at highest risk for contracting the disease. One sick person could infect dozens of others, as Woodring learned when he traced the root of 65 cases in one rural county to a man who had cared for his Ebola-stricken brother in Monrovia. That man returned home, got sick, and went to a bare-bones clinic. A grandmother from another village cared for him, wiping up vomit and comforting the man as he died overnight. The grandmother returned home and grew ill. Because she was a central and beloved figure in her community, dozens of people attended her funeral, caressing her body, kissing her—and contracting Ebola. Forty-seven of the infected people died, a 72 percent fatality rate.
“Honestly, all our efforts were for naught if we couldn’t control the burial system,” Woodring said. “Even though there is a huge science to Ebola, if you didn’t get people’s respect from the beginning—by offering it—you were just another white guy coming in telling them what to do.” He hopes national governments can harness the training and funding that followed the Ebola crisis to build sustained healthcare systems in the affected countries.
It’s an approach Elin Gursky, GSAS ’13, considers essential. In April, when United Nations Secretary General Ban-Ki Moon named a high-level panel to study the global response to health crises and present a report by the end of the year, Gursky was appointed to the resource group of experts supporting the panel. Broad and deep international cooperation and political will to invest more money in strong public health systems are what’s needed to prevent and counter future disease outbreaks, she said.
“You can bring in experts and surge capacities, but it needs to support, not supplant, local systems,” Gursky said. “It needs to start at the community level.”
When Laura Sida, a pediatric cancer nurse and a graduate student in Fordham’s master’s degree program in humanitarian affairs, arrived in Sierra Leone last spring, she thought she’d be part of a treatment clinic. But the work quickly shifted to disaster recovery. After six months spent helping ministry of health workers improve clinic management and supervising psychological and social support teams for Ebola survivors, Sida said recovering after the disaster is just as crucial for long-term health as responding to the crisis itself. She’s found her master’s thesis topic: the challenges of rebuilding after a disaster.
A particular difficulty in the aftermath of Ebola is that the disease attacks precisely the people who might be relied on to lead a social recovery, she said. “It kills the caretakers, the people who are the most caring and compassionate. So who is left? Ebola clears the household.”
How the countries build back, from the most immediate relationships in villages to the strength of national health systems—and what the international community learns from Ebola—will determine how the next global health crisis plays out. The world isn’t getting any less connected, as the few Ebola cases that emerged in the United States show, and there will inevitably be a next time, Van Tulleken said. “We need to understand that my life and the life of the poorest person in Africa are intimately linked.”
—Eileen Markey, FCRH ’98, is the author of a biography of Maura Clarke, one of the U.S. nuns killed in El Salvador in 1980, to be published next year by Nation Books.
]]>34296Lessons and Impacts of Ebola Outbreak Examined
https://now.fordham.edu/uncategorized/lessons-and-impacts-of-ebola-outbreak-examined/
Fri, 08 May 2015 16:00:00 +0000http://news.fordham.sitecare.pro/?p=16835Ellie Frazer, a master’s candidate in international political economy at Fordham
Last year’s Ebola outbreak may have faded from the headlines, but its economic impacts in West Africa and the troubling questions it raised about response efforts are far from resolved, according to panelists who have visited the African continent.
“We had more than 10,000 people die of Ebola, and Ebola should really be one of the easiest diseases to control,” said Dr. Alexander van Tulleken, the Helen Hamlyn Senior Fellow at Fordham’s Institute of International Humanitarian Affairs.
He was one three panelists at the April 24 event, “’Post-Ebola’ West Africa: Humanitarian Impact, Challenges, and Opportunities.” Van Tulleken described “an international system of pandemic response that doesn’t work,” noting that each Ebola case only generates about one other.
“The virus is not good at transmitting itself,” he said. “When you have one case in a Dallas hospital that led to several other cases of infected nurses, you then see both the lack of competence and the fear that even if we control Ebola—which we sort of managed to do—that a disease with a higher (transmissibility) like bird flu would really threaten the world economy and human life in a very significant way.”
Last year, the political risks and the risks of transmitting Ebola in various places around the world were not centrally managed, he said. The Obama administration’s Ebola “czar” was better qualified to address political risk than the “very small amounts of widespread risk” posed by the outbreak, he said.
The outbreak took a harsh toll on commerce and agriculture in Guinea, Sierra Leone, and Liberia, said panelist Ellie Frazier, a master’s candidate in the International Political Economy and Development program at Fordham. To illustrate, she pointed to the 2.8 percent drop in U.S. economic growth following the 2008 financial crisis, compared to an Ebola-related drop of 23 percent in Sierra Leone.
Also, response efforts call attention to “governance gaps” and poor access to justice-related services, she said, noting the barriers to women exercising their legal right to own and inherit land.
“You can come in and do an … economic recovery program and disperse seeds, but if your recipients don’t have secure access to land, where are those seeds going to go?”
She also emphasized the need to examine the conditions that allowed Ebola to spread.
In Sierra Leone, the country’s underdevelopment and a limited health infrastructure abetted the spread of the disease, said Ishmeal Alfred Charles, program director with Healey International Relief Foundation/Caritas Freetown in Sierra Leone.
He described his organization’s efforts to promote hand-washing—important because of the country’s lack of running water and a culture that favors touching as a means of expression. Also important was having burial teams dispose of corpses in a more dignified way, rather than simply enclosing them in bags and heaving them into trucks.
The piling of the still-contagious bodies on trucks “created a lot of risk because a lot of people were hiding at night, trying to bury their loved ones, and that created a lot of infection,” he said.
Van Tulleken said Ebola’s “high imaginability factor” was played upon in the news via graphic images, to the detriment of more useful information such as the need for public support of efforts to manage the epidemic in West Africa.
“Risk management is not a rational set of thought processes, it’s an emotional set of thought processes, and the media played on that to get a huge amount of news coverage for several months,” he said.
Held at Fordham Law School, the discussion was jointly hosted by Fordham’s Mellon Faculty Seminar on Humanitarianism, Department of Political Science, and Institute of International Humanitarian Affairs.
]]>16835More News on the Web …
https://now.fordham.edu/university-news/more-news-on-the-web/
Mon, 17 Nov 2014 19:45:39 +0000http://news.fordham.sitecare.pro/?p=44960 (Above and top right) On Nov. 9, the world recognized the 25th Anniversary of the fall of the Berlin Wall, and faculty and students who had visited Berlin offered perspective.
Karen Greenberg, Ph.D., director of Fordham Law’s Center on National Security, has examined parallels between the government’s response to the Ebola crisis and its response to terrorist threats.
Fordham held a daylong conference on the Bloomberg Era on Nov. 14.
Read all the stories at www.fordham.edu.
]]>44960IPED Student at Epicenter of the Ebola Crisis
https://now.fordham.edu/university-news/iped-student-at-epicenter-of-the-ebola-crisis-3/
Mon, 08 Sep 2014 20:47:04 +0000http://news.fordham.sitecare.pro/?p=45029The July 29 death of Sierra Leone’s top Eboladoctor, Sheikh Umar Khan, from the disease intensified the already high fears about the epidemic that is overwhelming Western Africa.
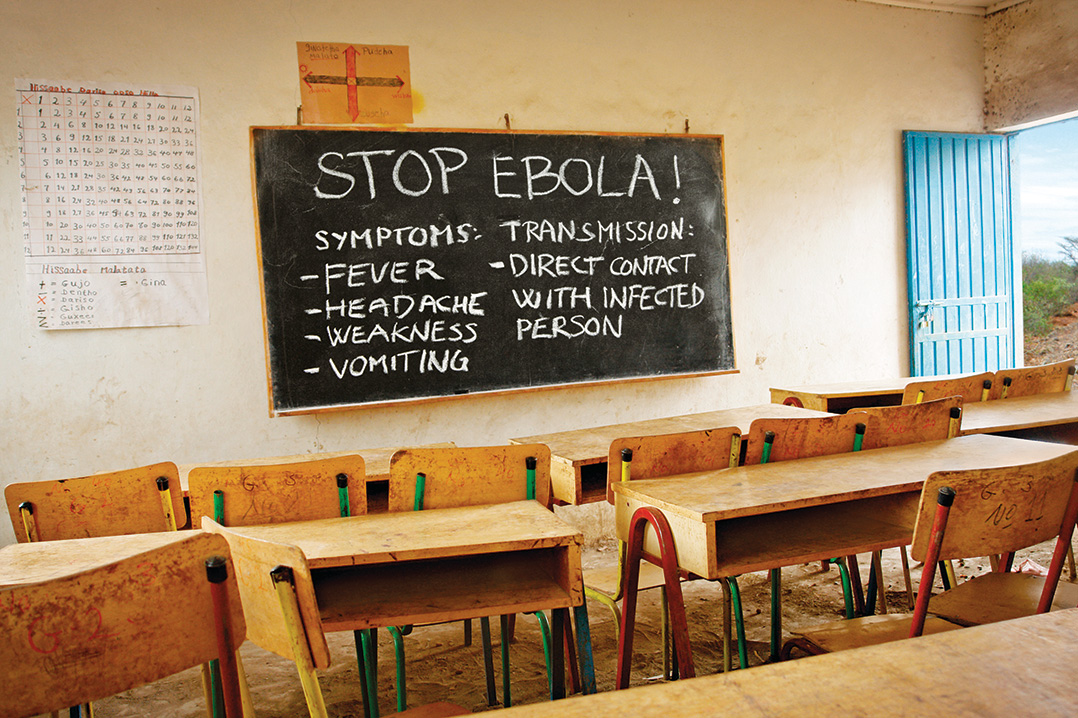
“On a daily basis, Ebola regularly comes up,” said Kathleen “Ellie” Frazier, a student in Fordham’s International Political Economy and Development (IPED) program who was working in Sierra Leone. “I overhear people discussing it on the street and there are awareness posters everywhere.”
Currently, Sierra Leone is the epicenter of an epidemic of the Ebola virus, which causes high fever, vomiting, diarrhea, and sometimes internal bleeding. The virus, for which there is no cure or vaccine, has a case fatality rate of more than 50 percent and remains infectious even after a person has died.
More than 3,069 cases and 1,552 deaths have been reported across West Africa (as of Aug. 28.) So far, 1,026 Ebola cases have been reported in Sierra Leone.
Frazier was stationed in a rural area of Sierra Leone as an intern at Timap for Justice, the country’s largest paralegal network. A former Peace Corps volunteer in Rwanda, she has worked extensively on social justice issues, especially in post-conflict regions. In Sierra Leone, she was working with Timap to develop organizational assessment tools and training materials, and was observing paralegal activities in its various offices.
She was there just a week when Ebola cases began to emerge.
“In the first week I arrived, Ebola was confirmed in the eastern part of the country, marking its departure from the original area along the eastern border with Liberia and Guinea,” she said. Initially, she hesitated about going to Timap’s rural offices. She even thought about leaving the country.
“But, with the exception of one mining company in the east, no one was evacuating their staff. The rural offices I was supposed to work in were not in the most heavily affected districts, so I decided to go.”
Frazier has not known anyone who has contracted the virus, although several Timap staff members fled a city with a major Ebola isolation unit after a prominent teacher there died. She said two of Timap’s offices in the east have been forced to temporarily suspend activities.
Frazier said that misinformation about the virus is rampant. Some Sierra Leoneans doubt it even exists, partly because Ebola symptoms are similar to the common diseases of malaria and Lassa fever. And there are some who insist the disease is a conspiracy, citing that the original contamination area is a stronghold of the opposition political party.
Conflicting messages early on from the World Health Organization (WHO) and Sierra Leone’s Ministry of Health and Sanitation caused further confusion, Frazier said. In more remote rural areas, villagers have even driven out WHO and Doctors Without Borders workers.
Fear also breeds misconceptions, she said. Because of the virus’ high contagion rate, those who test positive for Ebola are immediately transferred to an isolation unit, where loved ones cannot visit. If they die, their bodies are bagged and buried in a designated area, denying family members the opportunity to perform customary funeral rites. As a result, many people see going to the isolation ward as a “death sentence” and resist taking sick family members to health centers or hospitals.
“Some rumors go so far as to say that the wards are fronts for organ harvesting, or that they inject you with the virus once you are admitted,” Frazier said.
Frazier said that those affected by Ebola are facing discrimination. Health professionals are ostracized by friends and family because of their work with victims. Children from affected families have been driven away from school. People refuse to buy goods from affected families.
“Beyond individuals and families, it is likely that the districts most heavily affected will carry a stigma long after this outbreak subsides—whenever that may be.”
Frazier returned to the United States at the end of August.
— Joanna Klimaski Mercuri
For more on Ebola, see a Q and A with Fordham Professor Alex van Tulleken, M.D. on Fordham’s news site, www.fordham.edu/news.
]]>45029VIDEO: Poverty’s Role in the Ebola Epidemic
https://now.fordham.edu/politics-and-society/video-povertys-role-in-the-ebola-epidemic/
Tue, 26 Aug 2014 10:40:15 +0000http://news.fordham.sitecare.pro/?p=522Alex van Tulleken, M.D., the Helen Hamlyn senior fellow at Fordham’s Institute of International Humanitarian Affairs, is a physician who specializes in tropical diseases. He recently sat down to talk about the Ebola epidemic currently affecting West Africa.
What’s the biggest misconception about the Ebola virus?
In New York, the biggest misconception is that we’re likely to have an epidemic of Ebola here, or that you can catch it easily. People worry about Ebola because it has a very high case fatality rate. If you catch it, the chances of you dying are about 50 percent. That makes it pretty terrifying. The fact that it spread rapidly in West Africa also makes people think it could spread anywhere. It just isn’t the right kind of virus to do that. It’s actually not very contagious at all. It isn’t spread in an airborne mechanism, like flu. You really need contact with bodily fluids containing the virus.
This outbreak has been confined to Africa and is not expected to present a threat to U.S. citizens. Why should Americans pay attention?
This is killing a lot of people, but it is also destroying health systems. Which means that many more people are going to die of things other than Ebola. If we can’t contain a disease like Ebola, which isn’t that contagious, then it shows how hard it might be to contain something like flu. And if we were talking about flu, I would be saying that New Yorkers should be worried.
Why was it a greater threat to the populations of places like Sierra Leone to begin with, as opposed to the United States?
We’re talking about some of the poorest countries in the world. They’re different from America in almost every way. Many people can’t read and are poorly educated about health. There are a number of other cultural practices that are not helpful. One is the cultural practice of making contact with, and washing, the dead bodies; this sort of thing spreads disease.
Then there are the measures needed to control Ebola, like contact tracing. If we know you’ve got Ebola, we need to get in touch with everyone you’ve been in touch with. In New York, that’s pretty easy. But in West Africa it’s much, much harder. People are afraid of the health services. And many don’t have addresses and don’t have phones.
Does globalization make us more vulnerable to viral outbreaks?
Globalization is an important part of this conversation. We take more planes, there are higher densities of populations, and people move around more. But globalization is also one of the forces in which certain parts of the world have been excluded. We think of globalization as a force for good, and that as certain countries have become richer a rising tide has lifted all boats. In fact, in West Africa that has not been true. There hasn’t been consistent economic growth there for many decades. What we’re seeing now is a disease that’s really a hallmark of poverty and neglect.
Do you think this will serve as a wakeup call for the international community to provide more resources to prevention measures?
This will be a wakeup call in the short term, but the international community has a real problem when it comes to epidemic prevention, because no one ever won a medal for preventing an epidemic. You lose your job if you’re in the business of epidemic prevention, because people say well, there are no epidemics; we don’t need you.
How are relief agencies coping with the different crises around the world, such as Gaza, Syria, the Sudan, Ukraine, and now this?
The timing of the Ebola epidemic is really bad because ordinarily this would have been in the headlines months ago. When people started to say to the media that they’ve been reporting on this very poorly, they could for once reasonably say, ‘Look, there have been other things that have been really important. There are wars in Gaza, South Sudan, Syria,’ on and on it goes….
Is there room for optimism about these subjects?
The good news from the Ebola epidemic is that there is an incentive to develop vaccines and treatments, which in the long term will help—I don’t think we’re going to see a useful vaccine in this epidemic though, which I think will run for several months.
What we’re seeing are a group of aid organizations that are struggling to cope, that are poorly funded, and that are increasingly co-opted into political projects. Aid workers have been kidnapped or killed. So humanitarianism as it exists now is in a dangerous position. In the long run, to deal with humanitarian crises will require more training, more professionalism, and more money, and humanitarian organizations [will]require more room to work in a safe way.
]]>522Fordham Infectious Disease Specialist Talks to Media about Ebola
https://now.fordham.edu/politics-and-society/fordham-infectious-disease-specialist-talks-to-media-about-ebola/
Mon, 04 Aug 2014 15:30:56 +0000http://news.fordham.sitecare.pro/?p=39827As two Ebola-infected humanitarian healthcare workers are transported to Emory University in Atlanta for treatment, concern about a potential outbreak is heating up. Fordham’s Alexander van Tulleken has appeared on various media outlets to discuss whether such fears are warranted.
An infectious disease specialist and a senior fellow with Fordham’s Institute of International Humanitarian Affairs, van Tulleken has appeared on Al Jazeera America, MSNBC’s “Melissa Harris-Perry Show,” and locally, Fox-5 New York, with the same message:
“It’s very hard to catch this virus,” he says of Ebola, of which there is no cure, and causes hemorrhagic fever that kills at least 60 percent of the people it infects in Africa. Ebola spreads through close contact with bodily fluids and blood, meaning it is not spread as easily as airborne influenza or the common cold.
In this interview with New York’s Fox 5, he discussed the Ebola vaccine currently in trials, and also explained that the virus has been in the country for some time with the Center for Disease Control’s research. Watch here:
In this segment with MSNBC’s Melissa Harris-Perry, van Tulleken says that rather than worrying about a vaccine, “what we need to be doing is containing this epidemic in West Africa.” He also says prevention is always underfunded. “What we’re seeing is a failure of the international system to respond to this virus, and this is a virus we should care about for humanitarian reasons. These countries are really neglected, and that’s why it’s spreading.”
Image via NBC News
Watch both MSNBC segments below, and visit our YouTube page for more media appearances by van Tulleken and other Fordham faculty.
-Gina Vergel
]]>39827IPED Student at Epicenter of the Ebola Crisis
https://now.fordham.edu/politics-and-society/iped-student-at-epicenter-of-the-ebola-crisis/
Thu, 31 Jul 2014 06:53:13 +0000http://news.fordham.sitecare.pro/?p=539The July 29 death of Sierra Leone’s top Ebola doctor, Sheikh Umar Khan, from the disease intensified already-high fears about the epidemic that is overwhelming Western Africa.
“On a daily basis, Ebola regularly comes up,” said Kathleen “Ellie” Frazier, a student in Fordham’s International Political Economy and Development (IPED) program who worked this summer in Sierra Leone. “I overhear people discussing it on the street and there are awareness posters everywhere.”
Currently, Sierra Leone is the epicenter of an epidemic of Ebola, which causes high fever, vomiting, diarrhea, and sometimes internal bleeding. The highly contagious virus, for which there is no cure or vaccine, remains infectious even after a person has died.
More than 2,470 cases and 1,350 deaths have been reported across West Africa. So far, 907 Ebola cases have been reported in Sierra Leone.
Frazier was stationed in a rural area of Sierra Leone as an intern at Timap for Justice, the country’s largest paralegal network. A former Peace Corps volunteer in Rwanda, she has worked extensively on social justice issues, especially in post-conflict regions. In Sierra Leone, she worked with Timap to develop organizational assessment tools and training materials, and observed paralegal activities in its various offices.
She was there just a week when Ebola cases began to emerge.
“In the first week I arrived, Ebola was confirmed in the eastern part of the country, marking its departure from the original area along the eastern border with Liberia and Guinea,” she said. Initially, she hesitated going to Timap’s rural offices. She even thought about leaving the country.
“But, with the exception of one mining company in the east, no one was evacuating their staff. The rural offices I was supposed to work in were not in the most heavily affected districts, so I decided to go.”
Frazier has not known anyone who has contracted the virus, although several Timap staff members fled a city with a major Ebola isolation unit after a prominent teacher there died. She said two of Timap’s offices in the east have been forced to temporarily suspend activities.
Frazier said that misinformation about the virus is rampant. Some Sierra Leoneans doubt it even exists, partly because Ebola symptoms are similar to the common diseases of malaria and Lassa fever. And there are some who insist the disease is a conspiracy, citing that the original contamination area is a stronghold of the opposition political party.
Conflicting messages early on from the World Health Organization (WHO) and Sierra Leone’s Ministry of Health and Sanitation caused further confusion, Frazier said. In more remote rural areas, villagers have even driven out WHO and Doctors Without Borders workers.
Fear also breeds misconceptions, she said. Because of the virus’ high contagion rate, those who test positive for Ebola are immediately transferred to an isolation unit, where loved ones cannot visit. If they die, their bodies are bagged and buried in a designated area, denying family members the opportunity to perform customary funeral rites. As a result, many people see going to the isolation ward as a “death sentence” and resist taking sick family members to health centers or hospitals.
“Some rumors go so far as to say that the wards are fronts for organ harvesting, or that they inject you with the virus once you are admitted,” Frazier said.
Frazier said that those affected by Ebola are facing discrimination. Health professionals are ostracized by friends and family because of their work with victims. Children from affected families have been driven away from school. People refuse to buy goods from affected families.
“Beyond individuals and families, it is likely that the districts most heavily affected will carry a stigma long after this outbreak subsides—whenever that may be.”
UPDATE: As of Aug. 1, Frazier had left Sierra Leone and safely relocated to South Africa. She is scheduled to return to New York at the end of the month.
]]>539Fordham Student at Epicenter of Ebola Crisis
https://now.fordham.edu/politics-and-society/fordham-student-at-epicenter-of-ebola-crisis/
Wed, 30 Jul 2014 15:53:16 +0000http://news.fordham.sitecare.pro/?p=39835The July 29 death of Sierra Leone’s top Ebola doctor, Sheikh Umar Khan, from the disease has intensified fears about the epidemic that is overwhelming West Africa.
“On a daily basis, Ebola regularly comes up,” said Kathleen “Ellie” Frazier, a student in Fordham’s International Political Economy and Development (IPED) program who is working in Sierra Leone. “I overhear people discussing it on the street and there are awareness posters everywhere.”
Researchers are working to develop a treatment for Ebola, but right now there is no cure or vaccine. Infected patients receive only supportive care, such as saline and fever-reducing medication. Photo courtesy of BBC News
Currently, Sierra Leone is the epicenter of the Ebola outbreak, which causes high fever, vomiting, diarrhea, and sometimes internal bleeding. The highly contagious virus, for which there is no cure or vaccine, remains infectious even after a person has died.
More than 1,200 cases and 670 deaths have been reported across West Africa. So far, 454 Ebola cases have been reported in Sierra Leone.
Frazier is stationed in a rural area of Sierra Leone as an intern at Timap for Justice, the country’s largest paralegal network. A former Peace Corps volunteer in Rwanda, she has worked extensively only social justice issues, especially in post-conflict regions. In Sierra Leone, she is working with Timap to develop organizational assessment tools and training materials, and is observing paralegal activities in its various offices.
She was there just a week when Ebola cases began to emerge.
“In the first week I arrived, Ebola was confirmed in the eastern part of the country, marking its departure from the original area along the eastern border with Liberia and Guinea,” she said. Initially, she hesitated going to Timap’s rural offices. She even thought about leaving the country.
“But, with the exception of one mining company in the east, no one was evacuating their staff. The rural offices I was supposed to work in were not in the most heavily affected districts, so I decided to go.”
Frazier has not known anyone who has contracted the virus, although several Timap staff members fled a city with a major Ebola isolation unit after a prominent teacher there died. She said two of Timap’s offices in the east have been forced to temporarily suspend activities.
Image courtesy of BBC News
Frazier said that misinformation about the virus is rampant. Some Sierra Leoneans doubt it even exists, partly because Ebola symptoms are similar to the common diseases of malaria and Lassa fever. And there are some who insist the disease is a conspiracy, citing that the original contamination area is a stronghold of the opposition political party.
Conflicting messages early on from the World Health Organization (WHO) and Sierra Leone’s Ministry of Health and Sanitation caused further confusion, Frazier said. In more remote rural areas, villagers have even driven out WHO and Doctors Without Borders workers.
Fear also breeds misconceptions, she said. Because of the virus’ high contagion rate, those who test positive for Ebola are immediately transferred to an isolation unit, where loved ones cannot visit. If they die, their bodies are bagged and buried in a designated area, denying family members the opportunity to perform customary funeral rites. As a result, many people see going to the isolation word as a “death sentence” and resist taking sick family members to health centers or hospitals.
“Some rumors go so far as to say that the wards are fronts for organ harvesting, or that they inject you with the virus once you are admitted,” Frazier said.
Frazier said that those affected by Ebola are facing discrimination. Health professionals are ostracized by friends and family because of their work with victims. Children from affected families have been driven away from school. People refuse to buy goods from affected families.
“Beyond individuals and families, it is likely that the districts most heavily affected will carry a stigma long after this outbreak subsides—whenever that may be.”




 The July 29 death of Sierra Leone’s top Eboladoctor, Sheikh Umar Khan, from the disease intensified the already high fears about the epidemic that is overwhelming Western Africa.
The July 29 death of Sierra Leone’s top Eboladoctor, Sheikh Umar Khan, from the disease intensified the already high fears about the epidemic that is overwhelming Western Africa.
 ase specialist and a senior fellow with Fordham’s Institute of International Humanitarian Affairs, van Tulleken has appeared on
ase specialist and a senior fellow with Fordham’s Institute of International Humanitarian Affairs, van Tulleken has appeared on 


